Are Weight loss medications and bariatric surgery effective?
I often get asked for my opinion on weight loss surgery and weight loss medications. I think people suspect that because I’m so against diets, that I’m going to be against the surgery and medications that help people lose weight.
While I don’t recommend restrictive diets ever, I do support people who want to lose weight, and I do support surgery and medications in order to achieve that. Intentional weight loss, where appropriate (read: NOT for people with eating disorders), can be a very positive, health-focused change.
Weight loss may decrease all cause mortality and cardiovascular risk, reduce risk for type 2 diabetes, hypertension, and kidney disease, and improve mobility.
Not all of these things will apply to every person, of course, but denying that weight loss can have positive effects on our physical and emotional health doesn’t align with the research.
Do 95% of people who lose weight gain it back? The shocking truth about this often-cited statistic.
Importantly, losing weight in any way will not mend your relationship with food. Those issues need to be dealt with separately.
Weight is complex. It’s a given that the obnoxious ‘just eat less and move more’ suggestion for weight loss isn’t helpful. It’s a way someone who doesn’t have weight struggles, puts down someone who does.
If something as simple as eating less and moving more was really the answer, the weight loss industry would cease to exist. In reality, the reasons why people eat the way they do, are complicated.
Our weight and our ability to change our weight are determined by several things, including our genetics and our environment, and our socioeconomic status.
Here’s why we don’t all have the same 24 hours in a day.
For some people, for a variety of reasons, losing weight is really, really hard. They get to the point where they’ve exhausted all of their options outside of surgery and medication. Their weight becomes a health issue and a mobility issue, and all of their attempts at losing it begin to take a deep emotional toll.
To tell those people that weight loss surgery or medications are ‘taking the easy way out’ or ‘giving up,’ is not okay. It’s cruel, and it’s morally and intellectually wrong.
Our healthcare system does not treat fat people well, and neither does society. If we continue to tell people in larger bodies that their body size is all their fault and that they should be able to lose weight on their own, we then continue to cause these individuals both physical and emotional harm.
I also believe that those people who discourage intentional weight loss where it’s appropriate, are doing harm. If we strive for bodily autonomy for all, then part of that should be the decision to lose weight via whatever method is safe and effective.
I spoke to Jamie Mills, RDN, CD-N, a dietitian who has had weight loss surgery and is on social media as @thesleeveddietitian and on her site www.thesleeveddietitian.com.
This is her story:
I struggled with my weight my whole life. I was over 200 lbs by the time I was 10, and it never quite made sense since my family always had healthy foods and we were active kids. My sister never struggled the way I did. When I was 14 I was diagnosed with PCOS, and it started to make a lot of sense why I always struggled so much.
I tried every diet under the sun. In my early twenties I did successfully lose 70 lbs, however, that was achieved through some very unhealthy and disordered means. Because I had lost that weight by being so restrictive, I gained it all back. I finally decided that it was time for another tool, and that weight loss surgery was my best option to actually losing weight and managing my PCOS symptoms.
It’s hard to describe how awful it was being so overweight. Physically, I felt terrible. Getting out of bed hurt. Walking across campus to class and walking up stairs felt like an impossible task. I was so young (24 years old when I had my VSG) and here I was feeling completely trapped in my own body, despite always trying so hard. Not only was it physically uncomfortable, but mentally and emotionally I was in a terrible spot. My depression and anxiety was horrible, as was my self worth and body image. I didn’t socialize. I didn’t go out. I didn’t travel. I didn’t date. It was completely isolating.
What is weight loss surgery?
Weight loss surgeries in general involve creating a smaller space for food in the stomach, which limits the amount a person can eat.
There are several types of weight loss surgeries.
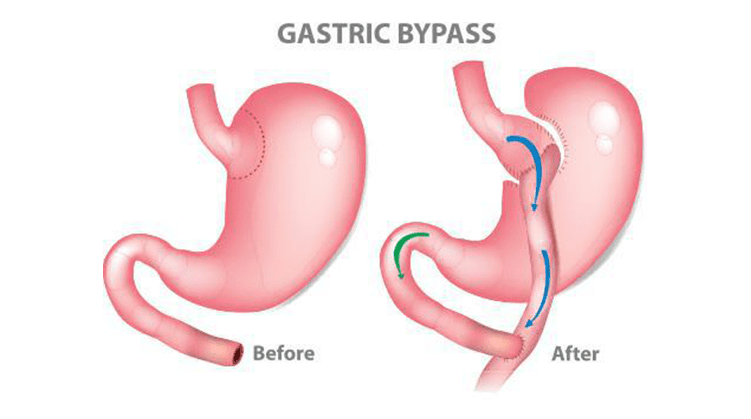
The most popular weight loss surgeries are the Roux-En-Y gastrectomy, otherwise known as gastric bypass, and the sleeve gastrectomy. In a Roux-En-Y, most of the stomach is removed, leaving a pouch around the size of a shot glass. The remaining portion is sutured to the middle part of the small intestine, called the jejunum.
The small size of the stomach severely limits the amount of food a person can eat, and bypassing the first part of the intestine, the duodenum, causes malabsorption of calories, vitamins, and minerals.
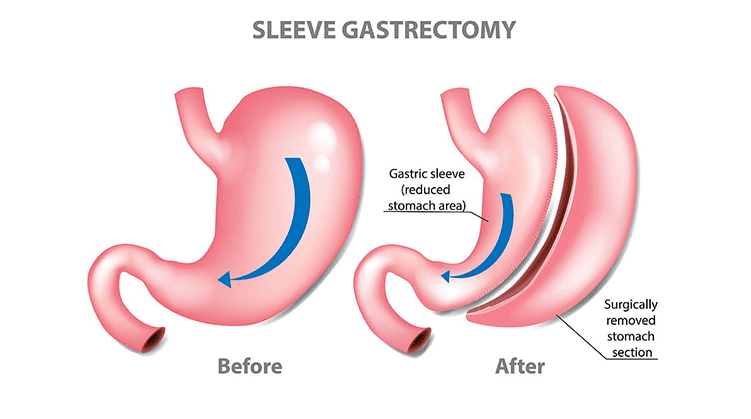
The Sleeve Gastrectomy is a procedure in which a large portion – 80-85% – of the stomach is removed, leaving a small pouch that connects as usual to the duodenum. With this surgery, the amount a person can eat is severely limited, but because the small intestine remains intact, they do not have malabsorption issues we see with the Roux-En-Y.
Weight loss surgery is not a small procedure. It needs to be done by an experienced surgeon, and you should be followed by a bariatric dietitian before and after the surgery. I’ve had patients who got the procedure in other countries, only to return to Canada and have major complications and no medical team to help them.
I asked Mills, who sees potential bariatric surgery patients, how she as an RD determines whether weight loss surgery is right for someone.
I think this is going to look different for each person. I think when your weight is affecting your health and quality of life, surgery and/or medication should at least be considered. Surgery will not be the right option for everyone, and not everyone will be a candidate. But in order to qualify most insurance companies require a BMI of 35 or more with comorbidities (high blood pressure, sleep apnea, high cholesterol, high blood pressure, etc) or a BMI of 40+ without comorbidities.
There are obviously more factors to consider, but if you fall into those categories and you continue to have unsuccessful attempts at weight loss with lifestyle changes alone, it would definitely be worth talking to your doctor about it.
I think people are so afraid to bring it up, or might not even think they would qualify, because it’s still so looked down upon. TLC shows make us believe you need to be 600lbs in order to have weight loss surgery, and that’s not the case. Weight loss surgery is the gold standard for treating obesity. Of all those who qualify, <1% actually receive the surgery.
I wish weight loss surgery could stop being used as a “last resort” option, and instead, be an option that is presented sooner. Why do we wait for health, mental health, and comorbidities to worsen before taking action?
While weight loss surgery is a permanent procedure, and one that should not be taken lightly, it is not nearly as risky as people assume. Risk for severe complications are 4% and risk of death from surgery is 1%. To put that into perspective, that’s about as risky as having an appendix removal.
Again, weight loss surgery will also not fix the psychological aspects behind your eating. If you’re consider weight loss surgery, please be sure that your team includes not only a dietitian, but also a psychologist or licensed counsellor to help you through the psychological tough spots.
Weight loss medications.
Medication for weight loss isn’t new.
Amphetamines like Dexedrine and Obetrol were widely used for weight loss in the 1960s and 70s. (Dexedrine is now prescribed for ADHD under the name Adderall).
The problem with amphetamines is that they’re very addictive, and can cause elevated blood pressure and psychosis. But by 1970, 9.7 million Americans used prescription amphetamines, and 3.2 million of these people were addicted to them.. Not all of these amphetamines were being taken for weight loss; they were prescribed for a multitude of conditions.
Once the government made amphetamines a schedule II drug, we mostly moved on from them for weight loss.
The next wave of weight loss drugs included phen-fen – a combination of dexfenfluramine and phentermine, and fenfluramine or dexfenfluramine on its own, which was sold under the trade name Redux or Pondimin. These were discontinued for their effects on the heart and several deaths that resulted from them.
Meridia’s story was similar – the drug, sibutramine, was found to cause heart problems and was pulled off the market in 2010.
Orlistat, which is still available as Alli and Xenical, works by causing the malabsorption of dietary fats. One of the side effects of this drug is oily stools, which can be avoided by eating a low-fat diet.
I think many people who are against weight loss medications feel that way because of the rather sordid history of these drugs. In addition, there’s still that feeling that fat people ‘should be able’ to lose weight without resorting to medications.
The newest weight loss drugs appear to be much safer, non-addictive, and effective. They work in a totally different way from the old-school uppers.
Weight loss drugs: the new class.
In 2014, the FDA approved the use of Contrave (naltrexone HCl and bupropion) for weight loss. You may have heard of bupropion in the form of Wellbutrin, a medication that’s commonly used for depression.
Naltrexone is a narcotic blocker that’s often used to block cravings in the treatment of alcohol and drug addiction.
Contrave works in the hypothalamus to reduce hunger, and in the mesolimbic reward system of the brain, to make eating less pleasurable.
The drug isn’t without its side-effects. Many users experience headaches, and the weight loss is minimal. The average weight loss with Contrave is around 5%, according to Spencer Nadolsky, D.O, who uses Contrave with patients for that purpose.
Because Contrave contains bupropion, it carries an increased risk for suicidal ideation, just like antidepressants that contain that same ingredient.
The latest weight loss medications are the GLP-1 receptor agonists are known by their trade names of Wegovy (semaglutide), Saxenda (liraglutide), and Ozempic (semaglutide).
GLP-1 comes from cells in our intestines. These medications work like our own GLP-1, slowing down gastric emptying, helping with insulin secretion and satiety, and improving blood sugar regulation. They also works in the part of our brain that increases satiety and possibly food cravings as well.
Nadolsky has noticed that way more than any drug, the GLP-1 receptor agonists help with binge eating. ‘People say, ‘I just feel normal now. I don’t feel like having second portions or snacking, and I don’t obsess over it.’’
Semaglutide was originally prescribed for the treatment of diabetes, but doctors quickly noticed that the medication seemed to result in weight loss at higher doses.
In 2021, semaglutide was studied at 2.4 mg for weight loss versus 1 mg for diabetes, and resulted in around 15% weight loss at that dose. It was subsequently approved specifically for weight loss.
Given once a week, the side effects of semaglutide are mainly nausea.
Lynn Smith (not her real name) has been overweight since she was 12 years old. Doctors have never found a physical reason why she struggled to lose weight, but there is likely a genetic component.
In her 30s, she realized there was an emotional eating component, so she did a year long program at Columbia University and lost a lot of weight. She kept it off for a couple of years, but the ‘hyper level of control’ and the 1200 calories a day weren’t sustainable.
Although Lynn has been working for 10 years with a therapist on her overeating (which is mainly resolved now), she has gained a lot of weight back during that time. She doesn’t eat emotionally anymore, and her diet is balanced. Still, she doesn’t comfortably fit into airline seats, chairs with arms, kayaks, and other confined spaces that most of us take for granted. She tore her achilles, so can’t do much exercise besides swimming.
For the past 1.5-2 years, Lynn has been on Ozempic and loves it. She hasn’t lost a great deal of weight, which may be due to her genetics. Still, she likes that she isn’t hungry as much, and is eating significantly less. She gets full faster, doesn’t think about food as much, and doesn’t have as many cravings.
‘It feels like a relief,’ she told me.
The latest medication, tirzepatide, seems to be the most effective GLP-1 agonist yet for weight loss, resulting in ‘substantial and sustained reductions in body weight’ in a 2022 trial.
‘Compared to the older drugs, these are much more effective,’ says Nadolsky. He says they have even better glucose lowering capability than even insulin.
He says that the effectiveness of these drugs ‘is basically turning into bariatric surgery in a medication. These drugs are amazing, but they’re extremely expensive, around $1000 a month.’ he says. And for some people, insurance doesn’t cover them.
The stigma around obesity is that insurance doesn’t want to cover people to lose weight. This is archaic and cruel, and just one more example of how people in larger bodies are treated unfairly by the medical system.
Weight loss medications aren’t a one-and-done situation, though. If people stop these drugs, they will regain the weight, says Nadolsky. ‘The chronic nature of obesity is that when we try to lose weight, the body fights back. You need to take these indefinitely.’
Check out Dr. Nadolsky’s clinic at joinsequence.com