What is The Best Diet for PCOS? Everything You Need to Know.
I’ve noticed a definite uptick lately in social media posts about PCOS. Some of them are legit. A lot of them aren’t. So I figured I’d step into the fray to give you the actual details about this condition, and arm you with the most current evidence around it.
A quick thank you to Spencer Nadolsky MD, Abbey Sharp RD (and on YouTube here), and Disha Narang, MD for being my experts throughout this post.
What is PCOS?
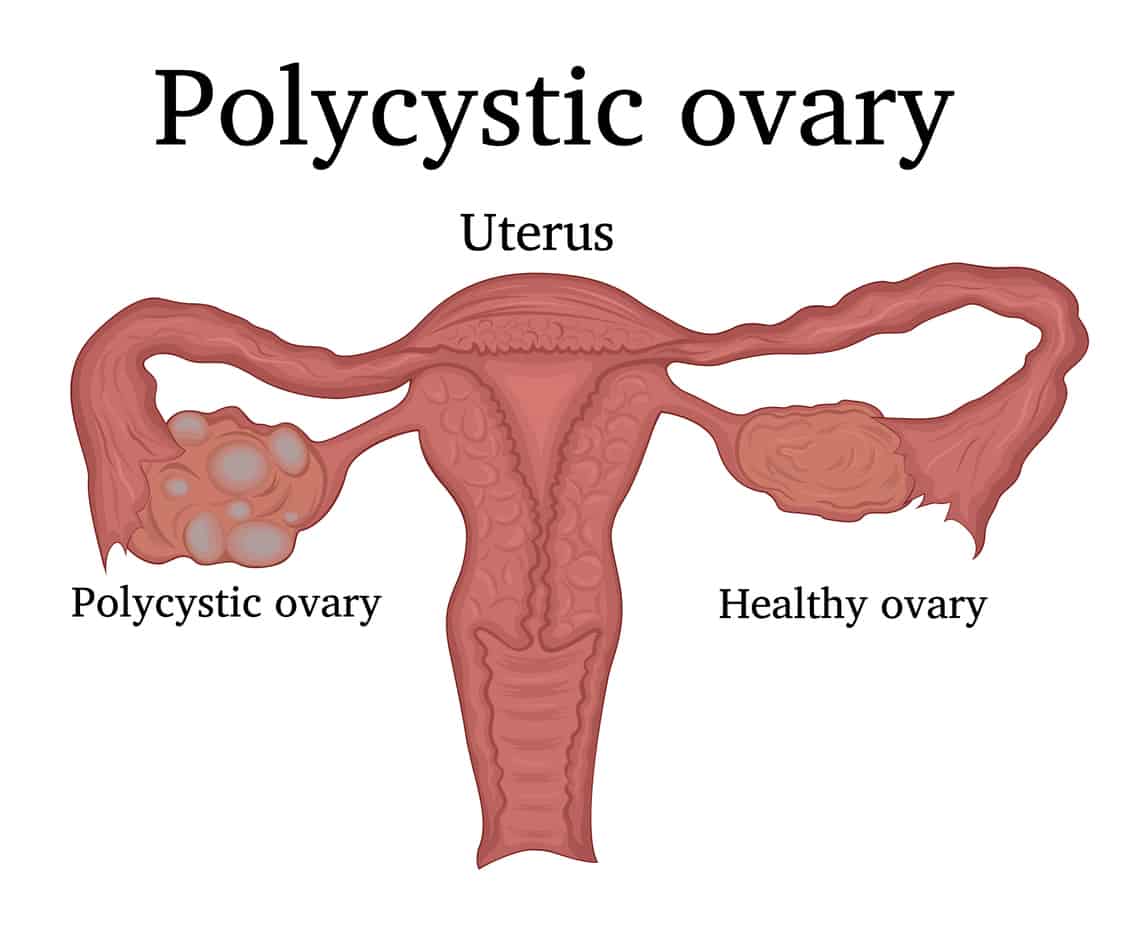
PCOS is a hormonal and endocrine disorder that occurs when the ovaries produce higher levels of androgens, than they do estrogens. It affects between 5%-10% of women of childbearing age.
The low levels of estrogens being produced mean that ovulation doesn’t occur.
Instead, the ovaries develop small cysts, which are really tiny fluid-filled follicles. Women naturally have follicles on their ovaries – they’re where immature eggs are kept. But women who have PCOS, have more than a normal number of antral follicles.
What normally happens, is that estrogen levels drop at the start of the cycle. The pituitary gland in the brain senses that and releases FSH, or follicle stimulating hormone. FSH does exactly that – it stimulates the growth of one follicle every month.
When the egg inside that one follicle matures, that egg is released during ovulation. This is the time in the cycle that estrogen peaks, and this surge of estrogen signals to the brain to dial it back on the FSH.
But in PCOS, because there are all these extra follicles, one single follicle doesn’t get enough FSH to grow. Instead, ovulation doesn’t occur. When ovulation doesn’t occur, estrogen isn’t released, and the brain doesn’t get the signal to stop it with the FSH.
Instead, the brain releases LH – luteinizing hormone – which makes testosterone. High levels of testosterone can cause many of the symptoms you see with PCOS, including hair growth, acne, and insulin resistance.
Women with PCOS appear to have a higher risk for developing heart disease, high blood pressure, diabetes, infertility, and endometrial cancer.
What are the causes of PCOS?
We don’t really know, unfortunately.
It seems to be genetic, at least in part.
And no, Epstein Barr has nothing to do with PCOS, sorry Medical Medium. Spread your garbage elsewhere. (Thank you, Natalie Crawford MD).
Diagnosis of PCOS
PCOS is diagnosed when someone has two of the following three symptoms:
- Irregular periods
- High androgen levels
- Ultrasound that reveals cysts
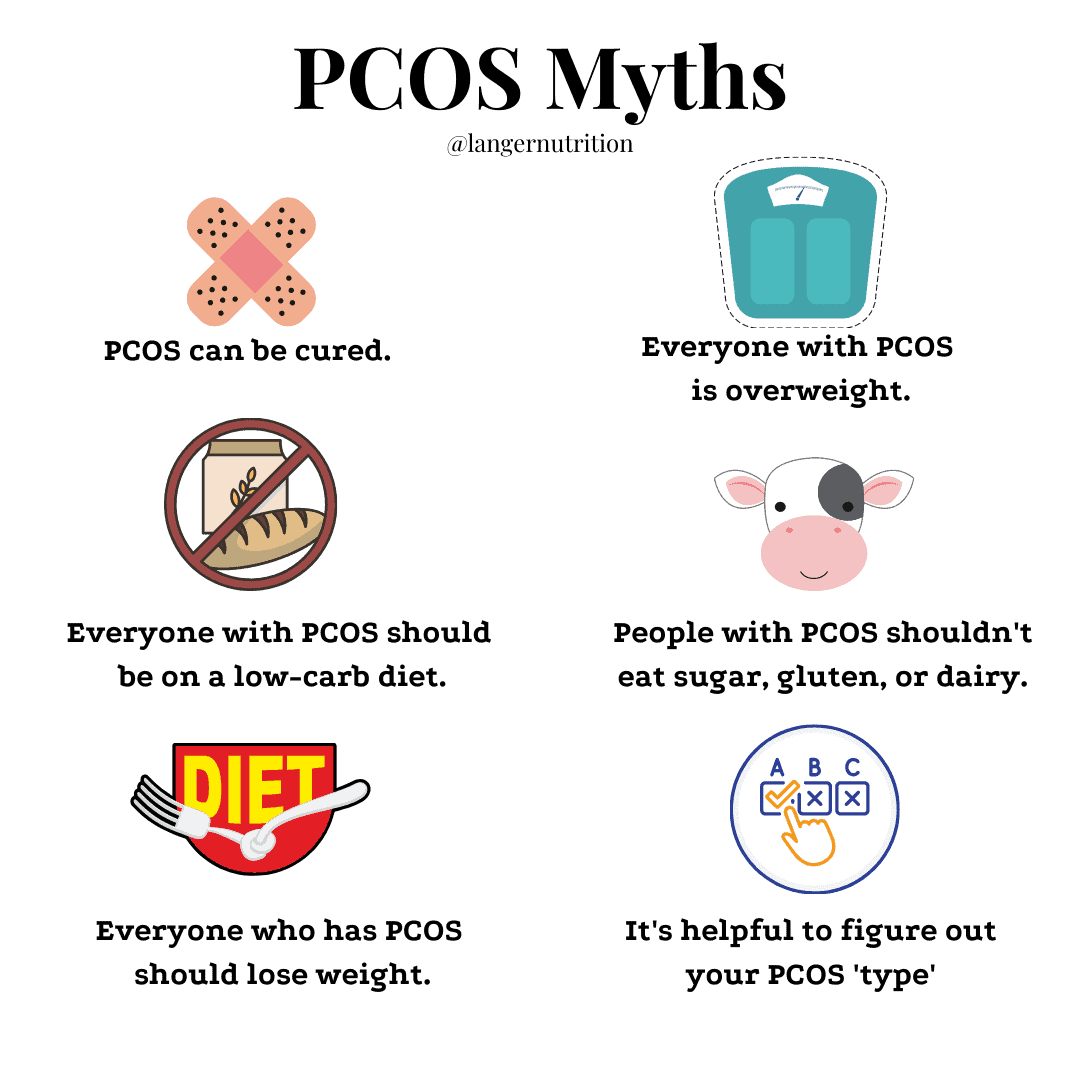
Unfortunately, PCOS is incurable. Beware of anyone who says they can cure your PCOS with a diet or supplements. No. No. No.
What are the symptoms of PCOS?
Low progesterone, which is a symptom of not ovulating.
High androgens, which can cause acne, hair loss, and increased hair growth on the face and arms. Note: not everyone who has hormonal acne has PCOS.
Women with PCOS are more likely to carry weight around their middles, because of the elevated androgens.
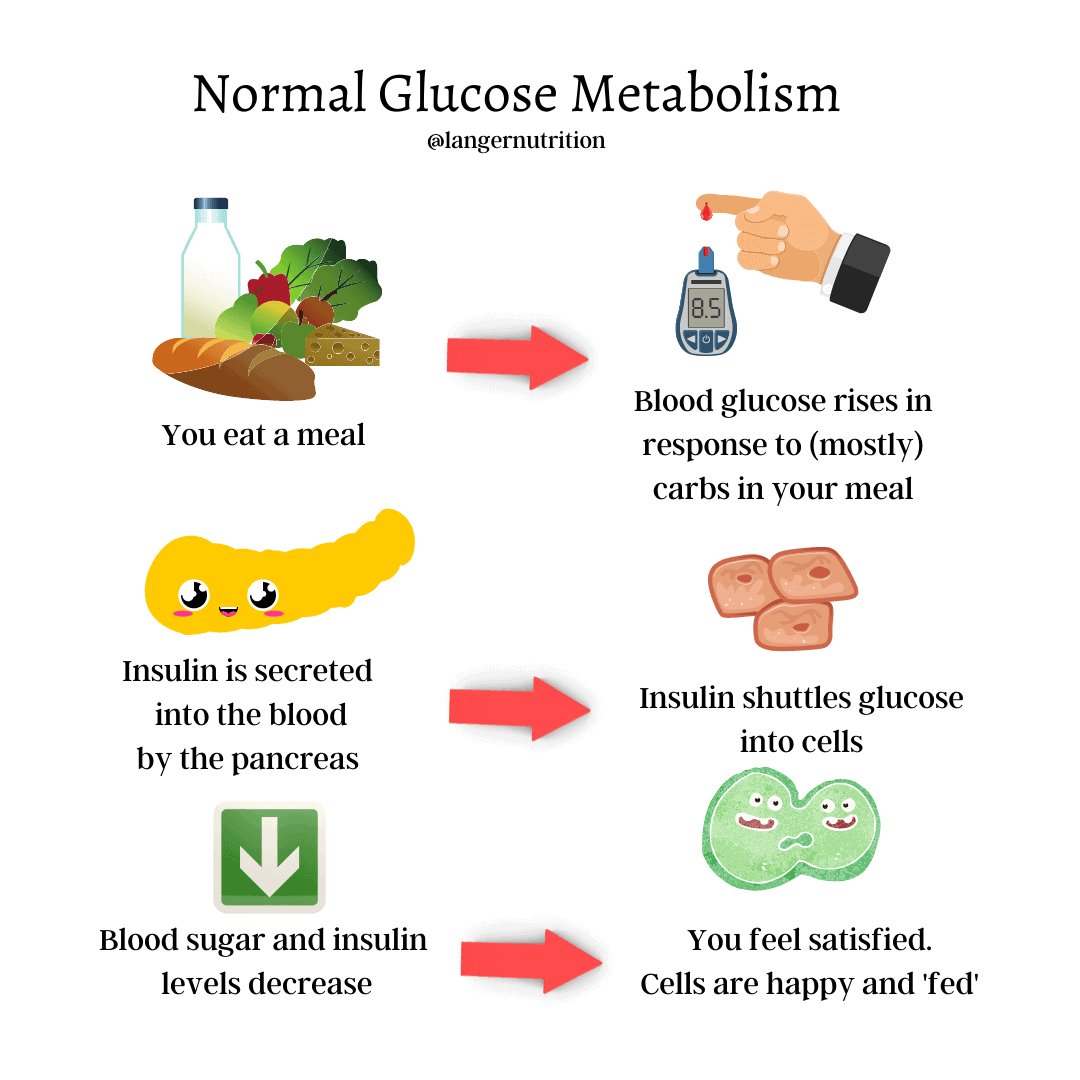
Insulin resistance. Insulin resistance seems to be one of the dominant factors in PCOS. Insulin resistance happens when our cells don’t respond to insulin the way they’re supposed to, so the pancreas releases larger amounts of it in a bid to regulate blood sugars.
The role of insulin is to shuttle glucose into the cells after we eat. If this isn’t happening, and the pancreas is pumping out insulin to try and mitigate the situation, we’re left with high blood levels of both glucose and insulin, which can cause issues.
First, the fact that the cells aren’t getting the glucose for energy that they need, can cause very intense cravings, especially for carbs. The cells are screaming for food, but they aren’t getting it, because the glucose is staying in the blood, not going into the cells where it belongs.
Second, the elevated insulin levels can trigger the production of androgens, which in turn, can stimulate appetite and weight gain (along with hair growth and acne).

And since we’re talking about cravings, cravings in PCOS can also be exacerbated by low levels of a hormone called CCK, which helps with satiety. And dysregulation of the hunger hormone, ghrelin, and satiety hormone, leptin, may also be present with PCOS.
Let’s do some simple math.
High insulin +
High androgens +
Low CCK +
Leptin and ghrelin dysregulation
______________
Cravings.
Not just any cravings, bad ones. And as with all cravings, strict dieting can make them worse.
When a person is being pushed and pulled by cravings and dieting, this may lead to binge eating. In fact, studies show that binge eating is prevalent in women with PCOS.
That’s unfortunately not a surprise.
Research suggests that women with PCOS have a higher risk for anxiety and depression, as well as eating disorders – around four to five times the normal rate.
Maybe that’s in part because so many doctors and other healthcare practitioners automatically prescribe weight loss diets for PCOS without really taking into account a person’s lifestyle or type of PCOS (more about that in a second).
In fact, during my research for this piece, I came across the weight-loss recommendation again and again and again.
It seems like the #1 piece of advice that everyone has for PCOS: just lose weight.
Yeah thanks, but it’s not so easy. And the likely result of this widespread advice is that the majority of people with PCOS have been on restrictive diets, and have weight cycled for a lot of their lives.
I can’t imagine being told for my entire adult life that I need to go on a diet. I can’t imagine the amount of shame and guilt I’d have every time an intense craving popped up and I couldn’t ignore it, because every one of my cells was screaming for glucose.
I also have trouble figuring out why restrictive weight loss diets would be a good idea for a condition that causes so many of the issues that diets also do:
Cravings. Check!
Inflammation. Check!
Weight gain. Check!
Hormonal fluctuations. Check!
People, Rome is already burning. Why are we going to pour gasoline on it?
If you’re having frequent intense cravings, eating more protein and fewer refined carbs, exercising more, and adjusting your medications may help.
PCOS and weight.
Between 40% and 80% of women with PCOS are classified as overweight. Not everyone with PCOS is overweight, which is a common myth.
It’s important to note that being overweight doesn’t cause PCOS – it can aggravate symptoms, however.
Weight gain with PCOS seems to occur, at least in part, because of insulin resistance.
As we discussed before, insulin resistance leads to a cascade of reactions that seem to increase weight: increased androgens, increased insulin levels, increased blood glucose.
Will weight loss help with your PCOS?
If you had symptoms of PCOS when you were thinner, weight loss is probably not going to change the situation.
Losing weight can sometimes – but not always – stimulate ovulation by getting rid of the fat cells that are secreting that extra estrogen, which lowers baseline estrogen levels.
Losing weight may also sometimes help with insulin sensitivity.
But going on a strict diet can also make things worse, physically and emotionally.
Should we treat the different types of PCOS differently?
There are different phenotypes of PCOS, and a lot of functional medicine practitioners make a big deal of how we should be treating each type differently.
The reality is that this is unnecessary – note that every site that has a quiz to find out ‘what type of PCOS you have’ seems to be run by a quack.
If the different types of PCOS really mattered, the literature would mention them a whole lot more. Don’t be distracted by people who feed you garbage just to sell you something.
What is the best diet for PCOS?
There is no diet that ‘cures’ PCOS. Rather, we manage symptoms and risk factors using both diet and sometimes supplements as well.
In fact, there is a paucity of research altogether around PCOS and diet. Even the broader topic of PCOS is still much of a mystery to us. There’s a lot we don’t know.
We do suspect that the following diet recommendations are helpful for PCOS:
A low-GI diet – aka a diet in which carbs are higher-fibre, slow-digesting (think, beans and lentils, whole grains) – does have some evidence suggesting that it may help with insulin sensitivity and menstrual irregularities.
Glycemic index can be a bit faulty as a tool, so what I recommend instead is just aiming for high-fibre, minimally processed carb choices most of the time.
Fibre may also decrease inflammation, improve satiety, and help with bloating. Don’t forget to drink lots of fluids when you increase your fibre.
Adequate protein: Protein helps with satiety. I recommend 25-30 grams of protein per meal. (Read more on how much protein we need every day, here).
Smarter carbohydrates: this means balancing your carbs with protein and fat to help slow glucose release into the bloodstream. It also means choosing slower-digesting carbs (like I recommended above).
Healthy fats: We suspect that high levels of saturated fats and of course, trans fats, increase inflammation. Unsaturated fats, on the other hand, like the ones in fish, avocados, and nuts, may decrease it.
Note: I know I say ‘may’ and ‘suspect’ a lot instead of ‘does’ and ‘know,’ but it’s extremely tough to establish causality in nutrition research, so making definite statements about whether X directly causes Y in most cases, isn’t something I’m prepared to do.
What probably doesn’t work for PCOS:
Gluten-free diets. *sigh* vilifying gluten AGAIN. There is zero evidence that gluten causes or worsens PCOS. Since this is the case, there’s no reason to remove it from your diet.
Dairy-free diets. There is no evidence that dairy causes any sort of PCOS issues. Some people might cite ‘inflammation’ as a reason to remove dairy – and gluten – from their diet, but unless you’re allergic or sensitive to these ingredients in the first place, not eating them is unlikely to cause inflammation, or help your PCOS.
Soy-free diets. No evidence, sorry.
Sugar-free diets. I know that a ton of people are pushing sugar-free diets for PCOS. And while I wouldn’t recommend eating a lot of sugar (even if you don’t have PCOS), never letting it touch your lips again is a bit extreme. Large amounts of sugar have been linked to inflammation, and with PCOS, you’re basically living in an inflammatory state.
How about keto and fasting for PCOS?
There’s a lot of information out there saying that people with PCOS should do keto and/or intermittent fasting to ‘cure’ their PCOS.
Intermittent fasting for PCOS.
IF may help with insulin resistance, but can cause blood sugar irregularities, especially if you’re the type of person who overeats after a fast. This can cause blood sugar spikes, which obviously aren’t what we want with PCOS.
And fasting is another way of cutting calories. But intense PCOS cravings may compounded when you cut calories, which honestly, sounds like two steps backward.
It’s important to note that the research is inconclusive in terms of whether fasting outperforms other methods of caloric restriction for metabolic markers (like insulin sensitivity and blood lipids).
Keto diet for PCOS.
There’s no compelling evidence that keto is a better way of eating for PCOS than the recommendations I gave above.
And we know that restrictive diets appear to be associated with more stress for the body, which again, you don’t need…especially with PCOS.
As far as the dietary interventions above are concerned, we don’t really know if it’s the diet itself, or the weight loss that may accompany it, that lead to positive effects on PCOS symptoms.
According to research and the International Evidence-Based Guideline for the Assessment and Management of Polycystic Ovary Syndrome 2018, there is no one superior diet pattern in the management of PCOS; they all have similar outcomes.
So for all of you who have asked me if you need to be on keto if you have PCOS?
Nope. You don’t.
For what not to eat, I recommend limiting ultra-processed foods and large amounts of sugar, which have been linked to inflammation.
Supplements for PCOS.
Always check with your pharmacist and doctor before starting any supplements.
Inositol.
Inositol is a sugar alcohol that’s readily found in nature, and is also produced from glucose by the human body. Myo-inositol is the form of inositol that is recommended to women with PCOS to help increase insulin sensitivity.
Inositol is the most well-studied of all the supplements recommended for PCOS, and the emerging research has been positive. (note: ‘emerging’ – this means we’re just starting to learn about it)
Studies suggest that 2000-4000mg of inositol a day may help with insulin sensitivity, fertility, and androgen levels.
Omega-3s.
There is some evidence that omega-3s may improve insulin resistance in women with PCOS, and lower levels of CRP (an inflammatory marker), testosterone, and blood lipids.
Other studies contradict some of these findings.
Probiotics.
We suspect that the gut microbiome and inflammation are linked. A 2016 study suggests that probiotics may have a positive effect on blood glucose, weight, and insulin sensitivity in women with PCOS. The strains of probiotic used in the study were lactobacillus and bifidobacterium, both of which are readily available.
Another 2019 study in the European Journal of Nutrition showed that probiotics and prebiotics reduced inflammatory markers in women with PCOS.
Vitamin D.
There is some evidence suggesting a link between low vitamin D status and some of the metabolic disturbances that occur with PCOS, including insulin resistance and high blood lipids.
This 2020 study in Gynecological Endocrinology and this 2018 study in Plos One establish that link, but more research is needed.
We don’t have all the answers around PCOS, but as research continues and we learn more, there will hopefully be newer, better ways to manage it.